Search
Aspergillus is increasingly associated with lung inflammation and mucus plugging in early cystic fibrosis disease during which conidia burden is low and strains appear to be highly diverse. It is unknown whether clinical Aspergillus strains vary in their capacity to induce epithelial inflammation and mucus production.
Cystic fibrosis (CF) is the most common chronic, life-shortening genetic condition affecting young Australians. There is no cure but researchers are working to prevent the onset of lung disease.

Rothwell Family Fellow; Head, Airway Epithelial Research

A promising new treatment pioneered in Western Australia for people with cystic fibrosis has commenced testing in a clinical trial in the United States and Australia.
The Kids Research Institute Australia spin-off company, Respirion, received $20 million in funding to develop a promising new therapy.
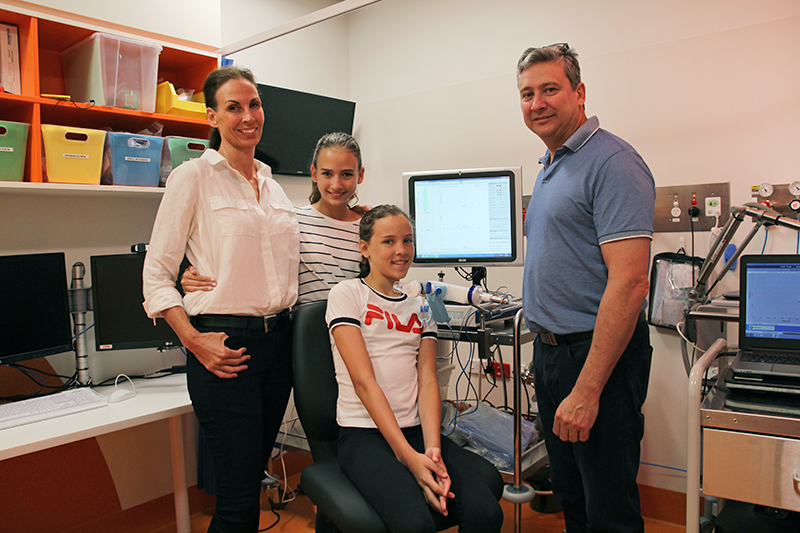
The family of two girls with cystic fibrosis are hopeful after The Kids Research Institute Australia spin-off company, Respirion, receives $20 million in funding to develop a promising new therapy.
A The Kids Research Institute Australia spin-off company has received $20 million from the Medical Research Commercialisation Fund to develop a promising new therapy for the treatment of Cystic Fibrosis.

PRAGMA-CF, a new way of measuring early lung disease in young kids with cystic fibrosis is changing the way we detect and treat CF.
When Ingrid Laing was born, the outlook for kids with cystic fibrosis was bleak. Her parents were told she might make it to 20 if she was lucky.

We are looking for 6 new members to join our Child and Adolescent Cystic Fibrosis Consumer Reference Group of WA